The Centers for Disease Control and Prevention has confirmed 62 cases of a post polio neurological condition called acute flaccid myelitis, also known as AFM. So far this year in the U.S. more than 90 percent of the cases involved children 18 or younger, with an average age of just 4 years old.
AFM is an illness that affects the nervous system, specifically the area of spinal cord called gray matter. It causes the muscles and reflexes in the body to become weak or even paralyzed. Cases of AFM are characterized by a sudden onset of arm or leg weakness and loss of muscle tone and reflexes.
Its symptoms are identical to those of poliomyelitis or polio which is associated with a so-called virus. Years of research have shown that these cases of polio and post-polio are associated with chemical poisoning or organochlorines used as a pesticide in farming found in all of our food sources (except for organically grown food).
Table 1: This graph shows polio in the United States in a context rarely (if ever) portrayed since Dr. Morton Biskind, the environmental context. [1] “DDT” and “DDT-like chemicals” are selected for this graph as the least complex way to represent a broad overview of the evolution of the technology of, and potential for, mass acidic chemical poisoning. (US Vital Statistics, US Government Printing Office, Washington, D.C.) [2][6]
Additional symptoms can include facial drooping or weakness, difficulty swallowing and slurred speech.
This condition, which may be caused by acidic poisoning from DDT like chemicals found in all non-organic fruit, vegetables, poultry and meat can lead to paralysis and even death, but no deaths have been reported so far this year.
Some prominent organochlorines are chlorobenzene, PCBs (polychlorinated biphenyls) and DDT (dichloro-diphenyl-trichloroethane). [3] Chlorobenzene is a precursor, a foundational compound used in the production of many industrial organochlorines as a chemical pesticide. [4] In the U.S., high production of chlorobenzene began in 1915, soon after the beginning of World War I. [5]
The above graph is a compilation of new cases per year (not incidence, as portrayed elsewhere herein). The data for the last half of the 20th century was gathered from U.S. Vital Statistics. [6] The very earliest numbers, from 1887 to about 1904, and the post polio numbers, are interpolated from the general historical commentary regarding those periods. [7] (see bibliography on Homepage and NYC Health Commissioner Haden Emerson’s compilations). While the graph is not perfectly accurate, due to changing methods of diagnoses and record-keeping within the medical system, it does give a reliable overall picture of Polio cases in terms of known literature and records.
The source for the U.S. and Swiss discoveries of paralysis in calves is from Van Nostrand’s Encyclopedia of Science and Engineering (1995), vol. 5, p1725. The phrase “Pesticides as a Panacea: 1942-1962” is a subtitle found in Encyclopedia Britannica, Macropaedia (1986). [8] Refer to other graphs (Overview) for specific pesticide comparisons with Polio incidence.
In 1915 Hooker Electrochemical began massive, unprecedented production of chlorobenzene (8,200 metric tons per year) and Dow Chemical began large-scale production soon thereafter. [9]
Chlorobenzenes are the basis for picric acid explosive used in World War I. [10] They have also been used in the manufacture of wood treatments, war gas, herbicides, insecticides, bactericide, moth control, and polymer resins. [11] (Mono) chlorobenzene is the base compound for DDT production. [12] Currently in the U.S., 15 million pounds of p- dichlorobenzene production goes into room deodorants. [13] According to Peter Duesberg, CDC’s investigation into Legionnaires disease ignored toxic chemical causes and created a new false field of study regarding the Legionella bacterium. [[4]
The sudden surge of chlorobenzene production coincides in time and place (1915, Niagara Falls) to be considered as probable cause for the epidemic of central nervous system diseases that followed the next year in the New York City region. [15] This epidemic lasted only six months, June to November, with 82% of the cases occurring in just 8 weeks. [16] While Polio literature terms this a world-wide Polio epidemic, it was peculiarly a phenomena of the U.S. and was especially prominent in the New York City region. [17] This is strange behavior for a supposedly so-called predatory Poliovirus, in an era, a continent, wholly unprotected by so-called miracle vaccines!
The number of new cases for 1916 (40,485) were calculated by multiplying the U.S. incidence rate by the U.S. population. [18] The number seems too high because of Naomi Rogers’ statements that worldwide new cases in 1916 were 27,000, that two-thirds of world Polio new cases were in the U.S. and that New York City new cases were 9,000. [19] While this discrepancy exists, the data is still useful for showing relative case numbers and/or incidence for the early 20th century. [See Tables 1,3,4,5,8,9,10 and 11]
Both Polio epidemics occurred two years after the beginning of World War I and World War II, if we use the dates of the epidemics, 1916 and 1942. [20]
DDT and “DDT-like chemicals” are used to represent the major organochlorine pesticides and organochlorines of similar neurotoxic character. [21] Most of the industrial organochlorines can produce CNS disease symptoms similar to Polio. [22] [Refer to Tables 2, 3, 5, 6, 7, 8, 9,10 and 11] below to see the relationship between DDT and DDT-like chemical production and the incidence of Polio.
Other Poisonous DDT-Like Pesticide Composite
Just over three billion pounds of persistent pesticides are represented in the Table 2 above and 3 below. Virtually all peaks and valleys correlate with a direct one-to-one relationship with each pesticide as it enters and leaves the US market. Generally, pesticide production precedes polio incidence by 1 to 2 years. The variation may be to variations in reporting methods and the time it takes to move pesticides from factory to warehouse, through distribution channels, onto the food crops and to the dinner table. A composite of these graphs, of the persistent pesticides–lead, arsenic, and the dominant organochlorines (DDT and BHC) is presented in Table 10.
The four chemicals were not selected arbitrarily. These are representative of the major pesticides in use during the last major polio epidemic. They persist in the environment as neurotoxins that cause polio-like symptoms, polio-like physiology, and were dumped onto and into human food at dosage levels far above that approved by the FDA. They directly correlate with the incidence of various neurological diseases called “polio” before 1965. They were utilized, according to Dr. Biskind, in the “most intensive campaign of mass poisoning in known human history.” [23]
Critique of Pesticides and Polio Vaccination
It certainly appears, from the above graphs, that the vaccination programs arrived a few years too late to be credited for declining polio case numbers. The programs were close enough, however, for media to shoehorn them into their historical position. This quote from Time Magazine (March 28, 1994) is a typical example:
“The great postwar epidemic peaked in the U.S. in 1952, when more than 20,000 children were paralyzed by polio and it tapered off in the early ’60s, after the Salk vaccine and then the Sabin oral version were introduced.” [23]
This smooth, loaded phrase, framed with glossy photos and clever captions, goes down like several shots of Vodka and with the same physiological effects. However, if we contain our admiration, and review the actual data, we realize that the great Polio epidemic actually occurred from 1942 (or gradually, beginning decades earlier) to 1962, that is, it was not a “postwar epidemic”. (Refer to Table 1) The epidemic declined not “in the early ’60s”, but a full decade earlier, in the early 1950s. Polio cases per year did not “taper off… after the Salk vaccine” as Time would have us believe — new cases per year dove resolutely downward two years before the Salk vaccine field trials and four years before the vaccination programs were firmly underway. The decline of Polio actually occurred after heated discussions regarding the dangers of DDT that began with in-house government/industry reviews of DDT in 1951, following Dr. Morton Biskind and other’s criticism of pesticides which began in 1945. [23 to 85] These discussions were followed by a phase-out through industry compliance, a huge shift of sales to third-world countries, a phase-in of less-persistent pesticides, which was facilitated by legislation in 1954 and 1956, (86) a renewed public image regarding the proper use and dangers of pesticides, [87] the cancellation of DDT registration by 1968, [88] and eventually the official ban of many of the persistent organochlorine pesticides by 1972 (in U.S. and developed countries). [89]
Notice that while pesticide production directly correlates with new polio cases per year through every peak and valley, the Salk vaccine enters only after Polio’s decline. (Refer to Tables 1 and 4) Salk’s point of entry is not sufficient evidence to be routinely offered as proof for the victory of vaccines over the Poliovirus, as Time implies, [90] and as implied by Hayes and Laws, [91] and virtually all other presentations of polio history in whatever media or educational forum.
The molecular biologist, Peter Duesberg, in his attempt to give Modern Medicine some credence with regard to virus causality (before refuting HIV causality with AIDS), [92] apparently felt he could assume, in Inventing the AIDS Virus, that, …the sudden, frightening polio epidemic that exploded in the Western nations, brought home by troops returning from the Pacific theater in 1945. [93]
Yet a glance at the graphs in Tables 1 and 4 shows his statement to be inaccurate. Polio was entrenched in the U.S. long before returning troops, and the increased Polio cases per year correlate much more consistently with pesticide production than returning troops. A rise in new cases per year that peaked in 1945 can be clearly attributed to the government’s release of war surplus DDT to the public market in 1945, not vague data about “troops returning from the Pacific theater in 1945”. The troops were heavily treated with DDT years before the U.S. civilian population and as can be expected, in light of the acidic chemical poison-theory, the troops suffered unusually high Polio incidence rates when compared to the non-treated populations where they were stationed, and soldiers based in the U.S.. [94] The unusual drama and rash assumption that fills this excerpt of Peter Duesberg’s writings gives a sense that he has taken the whole package of ingrained Polio images for granted. [95]
Pesticide Phase-Out and Vaccinations Phase-In
DDT and BHC were phased out from the developed nations and at the same time vaccination programs were dramatically credited with saving these countries from the ravages of the Poliovirus. (96) However, the banned pesticides continued with higher than ever total distribution in the under-developed countries thanks to W.H.O.’s anti-mosquito campaigns, where to this day acute flaccid paralysis (AFP), Polio, and DDT/BHC still prevail. (97) DDT application, DDT phase-out programs, and Polio vaccination programs are all being directed in these countries concurrently by the World Health Organization with little or no success. (98)
Registration for DDT was canceled in 1968, and DDT was banned by the EPA in 1972 — after the major organochlorines (DDT, BHC) had been gradually phased out of the U.S. market by the chemical industry and replaced with the less environmentally persistent pesticides, the organophosphates. (99)
Post-Polio Pesticides
In 1983, via new legislation, DDT was allowed back into the U.S. marketplace, but only in pesticide blends. (100) Within only a few months of this re-entry, a new kind of polio epidemic suddenly occurred. (101) It was labeled “Post-Polio”, the re-emergence of Polio symptoms in former victims. (102) This has involved approximately 600,000 victims and is shown in Table I above. Like most of the data, this correlation is not even a whisper in the mainstream media.
Central nervous system diseases other than Polio continues in the U.S. and throughout the world: acute flaccid paralysis, chronic fatigue syndrome, encephalitis, meningitis, muscular sclerosis, and rarely in humans, rabies. (103)
The harsh realities of government policy are stated in Casarett and Doull’s Toxicology (1996): “Although government agencies and industry have been slow in their re-evaluation of a vast array of pesticides in use, reassessment often comes in the wake of or concomitant with some recently disclosed adverse environmental or health effect.” (104) This after-the-fact approach to pesticide poisoning is puzzling enough without questioning Casarett and Doull’s careful usage of the words: “often”, “some”, “recently”, and “disclosed”. The acidic chemical environmental correlations of “Post-Polio are overlooked.
Searching PubMed has not been successful. However, an online a paper entitled “The Environmental Aspects of The “Post-Polio” Syndrome”, was found. This article establishes a strong correlation between environmental acidic chemical factors and “Post-Polio”. (105)
No other similar articles are to be found, and no abstracts were available, although it can be ordered from PubMed. Poliovirus presence in “Post-Polio” according to immunity and vaccination theories, if anyone should be immune to Polio, it should be former Polio victims, however, numerous studies of “Post-Polio” victims have found evidence of active Poliovirus. (106) (107) (108)
Polio images are projected as if this data doesn’t exist. It does not appear that money is being directed into these kinds of research studies.
Farr’s Law
Farr’s Law requires, for an epidemic to be a valid example of contagion, that the epidemic increase its incidence rates exponentially. (109) Since Polio has been ubiquitous since the beginning of human history, its incidence rate should have peaked long ago and universal immunity conferred, if immunity was ever required, and if the Poliovirus was actually a predator or even existed! Polio’s non-compliance with Farr’s Law is explained by viro pathologists with a unique argument, the inverse of the argument usually given to support so-called germ theory. (110) The argument is that the Poliovirus, which has been intimate with mankind since the beginning of history, suddenly became estranged from humans because of modern hygiene, and thus humans lost their natural immunity to the virus. (111) So it is modern hygiene and the resulting lack of exposure to the virus that is said to have caused the Polio epidemics to rage as never before. (112) It is interesting that for only one brief moment, viro-pathologists are willing to become eco-nutritional types who appreciate the value of natural breast feeding and the importance of the internal microbiological ecology conferred positively upon humans as I have suggested in my pH Miracle books and other published articles. (113)
Three different promotions of their inverse or perverse argument follows:
1) The prominent book on polio history by Naomi Rogers, where the inverse argument resides in the title, Dirt and Disease: Polio Before FDR. (114) The language style here is popular. (115)
2) In Textbook of Child Neurology (1995), John H. Menkes promotes the inverse argument with scientific language style: “Poliomyelitis… is less likely to be symptomatic in areas with inadequate sanitation, because poor sanitation is conducive to exposure at an age when lingering
transferred maternal immunity can attenuate the clinical picture.” (116)
3) In the propaganda film, A Paralyzing Fear: The Story of Polio in America. This was funded by the government and pharmaceutical firms and released in 1998. (117)
The New York Times (March 4, 1998) reviews the film. It reinforces the fundamental tenets of the Polio culture, beginning with a quotation from a section that portrays a “vintage film clip”: “My name is virus Poliomyelitis,” intones a cultivated, sinister male voice, as a camera pans over fair-weather clouds from which a hollow shadow emerges carrying the silhouette of a crutch. “I consider myself quite an artist, a sort of sculptor,” the voice continues. “I specialize in grotesques, twisting and deforming human bodies. That’s why I’m called The Crippler.”
Having dramatically demonized the Poliovirus, the medical cavalry rides to the rescue: …the epidemics grew steadily worse each year, with the number of new cases climbing from 5,000 in 1933 to 59,000 in 1952. (Refer to Tables 1 and 4)
Salvation came in 1954 with the Salk vaccine…And the inverse argument is now fit to print:
“The irony of the rise of polio in the 20th century, the movie reports, is that its prevalence was a result of improved sanitation. In grubbier times, babies and very young children developed antibodies to the disease, which had been around forever. A cleaner environment left increasing numbers of children with no natural immunity. (118)
So The New York Times review concisely presents the standard Polio images:
“the predatory virus, paralytic horror, epidemics, salvation via the Salk vaccine, and a unique exception from Farr’s Law.” (119)
I have my own personal concerns that anyone at NYT actually wrote this article, rather that it was probably supplied to the journalist as a suggested article, to be adjusted to the author’s style, thus essentially a customized press release.
The Epidemic Intelligence, Inventing The AIDS Virus (1996): The CDC’s disease-control mission was increasingly being regarded as obsolete, prompting serious discussions about abolishing the CDC altogether. (120) The situation changed in 1949 when the CDC brought on board Alexander Langmuir, an associate professor at the Johns Hopkins University School of Hygiene and Public Health. (121) Langmuir was the CDC’s first VIP, bringing with him both his expertise in epidemiology (the statistical study of epidemics) and his high-level connections — including his security clearance as one of the few scientists privy to the Defense Department’s biological warfare program……Langmuir and talked public officials and Congress into giving the CDC contingent powers to deal with potential emergencies… (122)
In July of 1951 he assembled the first class of the Epidemic Intelligence Service (EIS), composed of twenty-three young medical or public health graduates. After six weeks of intensive epidemiological training, these EIS officers were assigned for two years to hospitals or state and local health departments around the country. Upon completing their field experience, EIS alumni were free to pursue any career they desired, on the assumption that their loyalties would remain with the CDC and that they would permanently act as its eyes and ears. (123) The focus of this elite unit was on activism rather than research and was expressed in its symbol — a shoe sole worn through with a hole. According to British epidemiologist Gordon Stewart, a former CDC consultant, the EIS was nicknamed the “medical CIA.” (124)
Do YOU Believe the Polio Viral Theory?
The first isolation of a virus was achieved in 1892 by Russian bacteria hunter Dimitri Iwanowski, who gathered fluid from diseased tobacco plants. He passed this liquid through a filter fine enough to retain bacteria; yet to Iwanowski’s surprise, the bacteria-free filtrate easily made healthy plants sick. In 1898 a Dutch botanist, Martinus Willem Beijerinck, repeating the experiment, also recognized that there was an invisible cause and named the infectious agent “tobacco mosaic virus.” In the same year as Beijerinck’s report, two German scientists purified a liquid containing filterable viruses that caused foot-and-mouth disease in cattle (viruses were at one time called “filterable viruses,” but eventually the term “filterable” came to apply only to viruses, and was dropped). Walter Reed followed in 1901 with a filtrate responsible for yellow fever, and soon dozens of other disease-causing viruses were found.
In 1935 another American, Wendell M. Stanley, went back to the beginning and created pure crystals of tobacco mosaic virus from a filtered liquid solution. He affirmed that these crystals could easily infect plants, and concluded that a virus was not a living organism, since it could be crystallized like salt and yet remained infectious. Subsequently, bacteriologists all over the world began filtering for viruses, and a new area of biology was born-virology.
Historically, medical science has vacillated on the question of whether a virus is alive. Originally it was described as nonliving, but is currently said to be an extremely complex molecule or an extremely simple microorganism, and is usually referred to as a parasite having a cycle of life. (The term “killed” is applied to certain viral vaccines, thus implying an official conviction that viruses live.) Commonly composed of either DNA or RNA cores with protein coverings, and having no inherent reproductive ability, viruses depend upon the host for replication. They must utilize the nucleic acids of living cells they infect to reproduce their proteins (i.e., trick the host into producing them), which are then assembled into new viruses like cars on an assembly line. Theoretically, this is their only means of surviving and infecting new cells or hosts.
The Replicating Virus Theory
Then it was discovered that, when bacteria slowly begin to die, bacteria create tiny, apparently lifeless forms of survival, the so-called spores. It was then suspected that these spores were toxic and that they were the so-called pathogenic poisons. This was then refuted, since the spores are rapidly developing into bacteria when their vital resources are being restored. When scientists in the laboratory observed that the weak, highly inbred bacteria perished very quickly while turning into much smaller structures than the spores, it was first believed that the bacteria were being killed by the alleged pathogenic poisons, called viruses, and that the viruses were thereby replicating.
The Replicating Virus Theory
Then it was discovered that, when bacteria slowly begin to die, bacteria create tiny, apparently lifeless forms of survival, the so-called spores. It was then suspected that these spores were toxic and that they were the so-called pathogenic poisons. This was then refuted, since the spores are rapidly developing into bacteria when their vital resources are being restored. When scientists in the laboratory observed that the weak, highly inbred bacteria perished very quickly while turning into much smaller structures than the spores, it was first believed that the bacteria were being killed by the alleged pathogenic poisons, called viruses, and that the viruses were thereby replicating.
The Invention of Bacterial Viruses
Due to the belief that these – at the time of their discovery still invisible- structures were killing the bacteria, they were called phages/bacteriophages, “eaters of bacteria”. Only later it was determined that merely highly inbred and therefore almost non-viable bacteria can be made to turn into phages, or bacteria which are being destroyed so fast that they do not have time to form spores.
The introduction of the electron microscopy led to the discovery of the structures resulting from the biological transformation or pleomorphism of bacteria when these were suddenly dying or when the metabolism of the highly inbred germs was overwhelmed by processes triggered by the adding of “phages”. It was also discovered that there are hundreds of types of different-looking “phages”. The discovery of phages, the so-called bacterial “viruses”, reinforced the wrong assumption and the belief that there were human and animal viruses that looked the same and had the same structure. This is not and cannot be the case, for several different reasons.
After introducing chemical examination techniques in biology, it was discovered that there are thousands of types of phages and that phages of one type always have the same structure. They consist of a particular molecule, made of nucleic acid, which is covered in a shell of proteins of a given number and composition. It was only later discovered that merely the bacteria which had been highly inbred in the test tube could turn into phages themselves, by contact with phages, but this never applied to natural bacteria or bacteria which had just been isolated from their natural environment. In this process, it was discovered that these “bacterial viruses” actually serve to provide other bacteria with important molecules and proteins, and that the bacteria themselves emerged from such structures.
Before it could be established that the “bacterial viruses” cannot kill natural bacteria, but they are instead helping them to live and that bacteria themselves emerge from such structures, these “phages” were already used as models for the alleged human and animal viruses. It was assumed that the human and animal viruses looked like the “phages”, were allegedly killing cells and thereby causing diseases, while at the same time producing new disease poisons and in this way transmitting the diseases. To date, many new or apparently new diseases have been attributed to viruses if their origin is unknown or not acknowledged. This reflex found an apparent confirmation in the discovery of the “bacterial viruses”.
It is important to note that the theories of fight and infection were accepted and highly praised by a majority of the specialists only if and when the countries or regions where they lived were also suffering from war and adversity. In times of peace, other concepts dominated the world of science.[272]
It is very important to note that the theory of infection – starting from Germany – has only been globalized through the third Reich, when the Jewish researchers, most of which had opposed and refuted the politically exploited theories of infection, were removed from their positions.[273]
The Detection of Phages and Biological Transformation
The existence of phages can be proved rapidly
First step: their presence is confirmed through an effect, namely the transformation of bacteria into phages, and also through an electron micrograph of those phages. The control experiments show that phages do not appear if bacteria do not change or if bacteria randomly start decomposing due to extrinsic sudden annihilation, without forming phages.
Second step: the liquid containing the phages is concentrated and applied on another liquid, which has a high concentration at the bottom of the test tube and a low concentration at the top of the test tube. The test tube with the phages is then powerfully spun (centrifuged) and all the particles gather according to their mass and weight to the place of their own density. The density is the ratio of weight (mass) per unit of volume, expressed as Kg/l or g/mg, respectively. That is why this concentration and purification step for particles with the same density is called density gradient centrifugation.
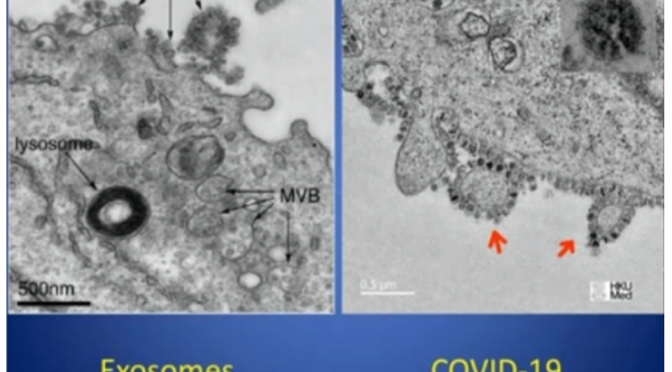
The layer where many particles of the same density gather becomes “cloudy”, which is called a “band.” This step is being documented, then the particles concentrated, purified and sedimented in a “band” are removed with a syringe needle. The extracted concentrated amount of particles is called an isolate. A fast and simple electron micrograph will confirm the presence of phages in the isolate, which at the same time is an indication for the purity of the isolate, if the micrograph shows no other particles but the phages. The appearance and the diameter of the phages will also be established with the help of this micrograph.
The control experiment performed for this step consists in treating and centrifuging the liquid from bacteria which did not form any phages, where no phages appear at the end of the procedure.
After the step of successfully isolating the phages, the decisive biochemical characterization of the phages follows. The biochemical characterization of their composition is essential for identifying the specific type of phage, since different types of phages often appear to be similar. The isolate obtained through the density gradient centrifugation is now divided in two parts. One part is used to determine the size, type and composition of the nucleic acid; in a separate procedure, the other part is used to determine the amount, size and morphology of the proteins of the phages. Since the 1970s, these tests have been simple standard techniques that are learned by every biology student in their first semesters.
These tests represent the biochemical characterization of the phages. In almost every case, these results have been and are being published in only one publication, since a phage has a very simple structure which is very easy to analyze. The control experiments for these tests use liquid from bacteria which do not form phages and thus cannot present any biochemical proof. The existence of approximately two thousand different types of phages have been scientifically demonstrated this way
The So-Called Pathogenic Viruses
The “bacteriophages,” correctly defined as incomplete mini spores and building blocks of the bacteria, have been scientifically isolated, while the so-called pathogenic viruses have never been observed in humans or animals or in their body fluids and have never been isolated and subsequently biochemically analyzed. To date, none of the researchers involved in virology research seems to have realized this very important point.
The use of electron microscopy and the biochemistry were very slowly returning to normal after 1945 and no one had realized that not one pathogenic virus had ever been isolated in humans or animals; thus, as of 1949 researchers started applying the same idea used for the (bacterio) phages, in order to replicate the human and animal “viruses.” John Franklin Enders, born in 1897 in the family of a rich financier, was active in various fraternities after having finished his studies, then he worked as a real estate agent and studied foreign languages for four years before turning to bacterial virology, which fascinated him. He then simply transferred the ideas and concepts that he learned in this area of research to the supposed pathogenic viruses in humans.
UnScientific Experiments and Interpretations Gave Birth to Virology
With his unscientific experiments and interpretations that he had never confirmed through negative controls, Enders brought the entire “viral” infectious medicine to a dead end. It is important to note at this point that Enders, like many infectious diseases specialists, worked for the U.S. military, which had always been and remains to date a huge victim of the fear of contagions. It was mainly the U.S. military which spread its erroneous belief that besides chemical weapons there were also biological weapons in the form of bacteria and viruses.
In 1949, Enders announced that he had managed to cultivate and grow the alleged polio virus in vitro on various tissues. The American expert opinion believed everything immediately. What Enders did was to add fluids from patients with poliomyelitis to tissue cultures which he claimed to have had sterilized, then he alleged that the cells were dying because of the virus, that the virus was replicating in this way and that a vaccine could be harvested from the respective culture. At that time, summer polio epidemics (polio = flaccid paralysis) were very frequent during summer and they were believed to be caused by the polio virus. A vaccine was to help eradicate the alleged virus. After the polio vaccine was introduced, the symptoms were then re-diagnosed among other things as multiple sclerosis, flaccid acute paralysis, aseptic meningitis etc. and later polio was claimed to have been eradicated. During his experiments, Enders et al. sterilized the tissue cultures in order to exclude the possibility of bacteria killing the cells. What he didn’t take into consideration was that the sterilization and the treatment of the cell culture when preparing it for the alleged infection was exactly what was destroying and killing the cells. Instead, he interpreted the cytopathic effects as the existence and the action of a so-called polio virus, without ever having isolated a single virus and describing its biochemistry. The necessary negative control experiments, which would have shown that the sterilization and the treatment of the cells prior to the “infection” in the test tube was killing the cells, have never been performed. However, for this “performance” Enders received the Nobel prize in 1954.
The Invention of the Polio Virus and ‘YES” the Measles Virus Too!
1954 is also the year in which Enders applied and introduced the same technique in order to allegedly replicate the measles virus. As he had been awarded the Nobel prize for the alleged polio virus the same year, all researchers believed his technique to be scientifically valid. Thus, to date, the entire concept of polio and measles has been based upon this unscientific technique and fraud.
Thus, the polio and measles vaccines do not contain viruses, but particles of dead monkey kidney tissue or human cancerous body cells. To date, no negative control experiments have been done with respect to the so-called polio and measles viruses either, which would have shown that it was the laboratory procedures that lead to the cytopathic effects on the cells.
Additionally, all claims and experiments made by Enders et al. and subsequent researchers lead to the only objective conclusion, that in fact they were observing and analyzing the cellular particles or fragments and the activity thereof in the test tube, misinterpreting these as particles and characteristics of the alleged polio and/or measles viruses.
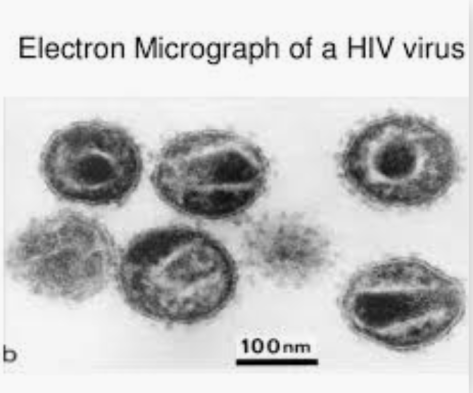
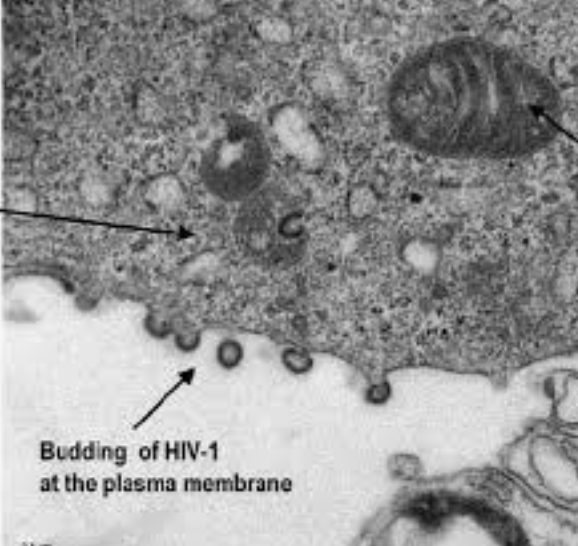
ALL Viruses from HIV, EBV, CMV, Hepatitis C, West Nile Virus, Ebola, Zika Virus, etc. are ALL Phantom Viruses
Their Existence Has NEVER Been Scientifically Demonstrated!
The following explanations applies to all the so-called (human or animal) “pathogenic viruses”. The six papers provided by Dr. Bardens in the course of the “measles trial” as proof for the existence of the measles virus described in a didactically ideal way the various steps of the chain of misinterpretations up to the belief in the existence of a measles virus.
The first paper was published in 1954 by Enders et al.: “Propagation in tissue cultures of cytopathogenic agents from patients with measles” (Proc Soc Exp Biol Med. 1954 Jun; 86 (2): 277–286).
This publication can be found on the internet, like all the other publications presented at the measles trial. In that experiment, Enders et al. cut down dramatically on the nutrient solution and added cell-destroying antibiotics to the cell culture before introducing the allegedly infected fluid. The subsequent dying of the cells was then misinterpreted as presence and also isolation of the measles virus. No control experiments were performed to exclude the possibility that it was the deprivation of nutrients as well as the antibiotics which led to the cytopathic effects.
Enders’ and his colleagues’ blindness can be explained by the fact that he truly wanted to help people, while the ‘virus hysteria’ was intensifying after the war and during the cold war. It can also be explained by the fact that Enders and many of his colleagues had no idea about medicine or biochemistry and they were competing with the Soviet Union for the development of the first measles vaccine. Such a pressure for success can also explain why Enders and his colleagues ignored their own reservations and cautions expressed in 1954, when they had observed and noted that many cells also died after being treated normally (i.e. without being “infected”), which they thought to have been caused by unknown viruses and other factors. All these facts and cautions were subsequently disregarded.
The second paper presented by the claimant in the ‘measles trial’ was published in 1959[274] and, for the reasons presented above, the authors concluded that the technique introduced by Enders was not appropriate for the isolation of ANY virus. This rebuttal is not only NOT being discussed by ALL the other researchers, but it is being ignored completely!
The ‘Viral Dogma’ of Pathogenic Viruses is Still Being Promoted Today!
In a third paper[275], the authors photographed typical cellular particles inside the cells and misinterpreted these as measles virus. They did not isolate any virus. For unexplained reasons, they failed to determine and describe the biochemical structure of what they were presenting as a virus in a separate experiment. In the short description of the methods used, one can read that the authors did not apply the standard isolation technique for viruses, i.e. the density gradient centrifugation. They simply centrifuged fragments of dead cells at the bottom of a test tube and then, without describing their biochemical structure, they misinterpreted the cellular debris as viruses.
From the way the experiments were performed, one can only conclude that cellular particles were misinterpreted as viruses. We find the same situation in the fourth[276] and the sixth[277] publication put forward by the claimant as proof of the existence of a measles virus. The fifth publication[278] is a review describing the consensus process as to which nucleic acid molecules from the dead cells would represent the so-called genome of the polio or measles virus. The result is that dozens of research teams work with short pieces of cell-specific molecules, after which -following a given model – they put all the pieces together on paper. However, this jigsaw puzzle made of so many pieces was never scientifically proven to exist as a whole and was never isolated from a virus, for a polio, measles, HIV or Hepatitis C, Ebola or Zika viruses have never been seen, neither in humans nor in a test tube. Referring to this publication, the court-appointed expert stated that it described the gold standard, i.e. the entire virus genome. It is obvious that the expert did not read this paper, whose authors stated that the exact molecular composition and functions of the measles virus genome will have to be the object of further research, which is why they had to rely on other virus models in order to achieve a consensus on the structure and functions of ANY virus genome. The easiest thing for anyone to notice is that in all of these publications, as well as in all other publications on the “measles virus” and other pathogenic viruses, including HIV, EBV, CMV, Ebola and Zika, no control experiments have ever been performed. No researchers used the density gradient centrifugation technique; instead, they only centrifuged cellular debris at the bottom of a test tube. This technique, used to collect all the particles from a fluid, is called pelletizing. From a logical and scientific perspective, it can be said that in all publications on the so-called “pathogenic viruses”, the researchers demonstrated in fact only particles and characteristics of cells. I would also like to point out that the so-called giant viruses[279] , i.e. an enwrapped nucleic acid can be found everywhere in the sea and in basic organisms. Like all bacterial phages, not only are they harmless, but they have beneficial functions. They can be also isolated by using the density gradient centrifugation, which proves their existence (see the graphic above).
I also recommend Prof. Lüdtke’s relevant review (1999).[280] He noted that at the early beginnings of virology, the majority of virologists always concluded that the structures they had mistaken for viruses turned out to be components of the cells and thus, they were only the result of the experiment and not the cause of the changes observed.
After the discovery and characterization of the phages and after introducing the dogma that the nucleic acid was the genome of all cells and viruses, the consensus was born, according to which such viruses must exist in humans and animals as well. In 1992, the dogma stating that the nucleic acid is the genotype of all cells was retracted in the scientific community. The ‘viral dogma’ of pathogenic viruses, however, is still being promoted today to the harm of billions of people. – for what?
The Bottom Line Concerning Phantom Viruses and the Polio Virus
My bottom line still holds the truth that the terrain or internal environment is everything and the germ or so-called virus is NOTHING! The germ or so-called virus can only be a symptom of cellular breakdown due to an imbalance of the delicate alkaline pH balance of the body fluids and NOT the cause of that breakdown. That is why years ago I offered any scientist in the World a finders fee of 5 million US dollars if they could prove the existence of the HIV virus using Koch’s postulates. It has now been over 20 years and I am still waiting even though currently I no longer have the funds to pay the prize due to political assassination! It is unfortunate that a former 5 million US dollar prize offered 20 years ago was not enough money to change the current medical viral dogma that is currently paying out trillions of dollars to guess who?
Click here to read more: http://medcraveonline.com/IJVV/IJVV-02-00032.php
To order your copy of Second Thoughts About Viruses, Vaccines and the HIV/AIDS Hypothesis go to: https://www.amazon.com/…/ref=dbs_a_def_rwt_hsch_vapi_taft_p…
Lecture in Dubai – The Annual Conference on Bacterial, Viral and Infectious Diseases
http://www.drrobertyoung.com/events.html
Join Robert O Young PhD and Galina Migalko MD in Dubai on December 5th and 6th, 2018 for the Annual Conference on Bacterial, Viral and Infectious Diseases. They will be Key Note Speakers and doing a workshop on the New Biology.
For more information and to register go to: https://bacterialdiseases.infectiousconferences.com/organiz…
The following is the abstract for Dr. Young’s lecture:
The Dismantling of the Viral Theory
Robert O Young CPT, MSc, DSc, PhD, Naturopathic Practitioner
Abstract
There is now over 100 years of documented history and research on the Polio virus and whether or not its treatment by inoculation has been successful in eradicating Polio. I am suggesting in this article and in my lecture that there are significant findings based on historical and past and current research, including my own that the viral theory of Polio and possibly other modern-day diseases, such as Post-Polio Syndrome, Polio Vaccine-Induced Paralysis, Legionnaires, CNS disease, Cancer, HIV/AIDS and now Zika may be caused by acidic chemical poisoning from DDT (dichloro-diphenyl-trichloroethane) and other related DDT pesticides, acidic vaccinations, and other factors including lifestyle and dietary factors rather than from a lone infectious virus. I will present ten historical graphs outlining the history of Polio, the production of DDT, BHC, Lead, Arsenic, Polio vaccinations and the author’s theory that chemical poisoning, vaccination, and lifestyle and dietary choices are a more likely causes for the symptoms of Polio, neurological diseases, Cancer, HIV/AIDS and now Zika.
https://www.linkedin.com/…/lecture-dubai-annual-conference…/
https://bacterialdiseases.infectiousconferences.com/organiz…
References:
[1] Morton S. Biskind, MD. “Public Health Aspects of the New Insecticides”. American Journal of Digestive Diseases, New York, 1953, v 20, p331.
[2] Handbook of Pesticide Toxicology, edited by Wayland J. Hayes, Jr. and Edward R. Laws, Academic Press Inc., Harcourt Brace Jovanovich, Publishers, San Diego, 1991, p769
[3] Toxicological Profile: for DDT, DDE, and DDE. Agency for Toxic Substances and Disease Registry, September 2002.
[4] U. Beck, E. Löser “Chlorinated Benzenes and other Nucleus-Chlorinated Aromatic Hydrocarbons” Ullmann’s Encyclopedia of Industrial Chemistry, 2012, Wiley-VCH, Weinheim.
[5] Chlorobenzene”. Immediately Dangerous to Life and Health. National Institute for Occupational Safety and Health (NIOSH)
[6] U.S. Vital Statistics, U.S. Government Printing Office, Washington, D.C.
[7] Historical Statistics of the U.S., The U.S. Government Printing Office, Washington, D.C.
[8] Van Nostrand’s Encyclopedia of Science and Engineering (1995), vol. 5, p1725. The phrase “Pesticides As A Panacea: 1942-1962” is a subtitle found in Encyclopedia Britannica, Macropaedia (1986).
[9] Thomas, Robert E. (1955), Salt & Water, Power & People: A Short History of Hooker Electrochemical Co. Niagara Falls, NY: Hooker Chemical Co.
[10] Booth, Gerald (2000), “Ullmann’s Encyclopedia of Industrial Chemistry – Nitro Compounds, Aromatic”. doi:10.1002/14356007.a17_411. ISBN 3527306730
[11] Weber, Manfred; Weber, Markus; Kleine-Boymann, Michael (2004). “Ullmann’s Encyclopedia of Industrial Chemistry – Phenol”. doi:10.1002/14356007.a19_299.pub2. ISBN 3527306730.
[12] Haller, H. L., Bartlett, P. D., Drake, N. L., and others: The Chemical Composition of Technical DDT, American Chemical Society, Journal, volume 67, pages 1591- 1602, 1945.
[13] Jo-Yu Chin, Christopher Godwin, Chunrong Jia, Thomas Robins, Toby Lewis, Edith Parker, Paul Max, and Stuart Batterman, “Concentrations and Risks of p-Dichlorobenzene in Indoor and Outdoor Air,” Indoor Air, 2013 Feb; 23(1): 40–49, Published online 2012 Jul 18. doi: 10.1111/j.1600-0668.2012.00796.x.
[14] Duesberg, PH, “Inventing the AIDS Virus,” Regnery, (1996). ISBN 0-89526-399-8. [15] Icon Group International (Author), Chlorobenzene: Webster’s Timeline History, 1851 – 2007 May 17, 2010
[16] Ibid [17] Ibid
[18] Risse, GB (1988). Fee E, Fox DM, eds. Epidemics and History: Ecological Perspectives. in AIDS: The Burden of History. University of California Press, Berkeley. ISBN 0-520-06396-1.
[19] A Disease of Cleanliness: Polio in New York City, 1900-1990, in David Rosner, ed., Hives of Sickness: Public Health and Epidemics in New York City Rutgers University Press, 1995, pp. 115-130.
[20] McDonough, F., The Origins of the First and Second World Wars (Cambridge Perspectives in History), Cambridge University Press, August 28, 1997.
[21] Goel, A, Aggarwal, P, “Pesticide Poisoning,” Natl Med J India. 2007 Jul-Aug; 20(4):182-91.
[22] Ibid.
[23] Biskind, MS (1953) “Public Health Aspects of the New Insecticides,” American Journal of Digestive Diseases 20: 331-341.
[24] TIME Magazine, U.S. Edition, March 14, 1994 Vol. 143 No. 11. [25] Baily, J. W.: J. Am. Vet. M. A. 113: 251, Sept. 1948.
[26] Biden-Steele, K. and Stuckey, R. E.: “Poisoning by DDT Emulsion: Report of a Fatal Case”, Lancet, 2: 235-236, Aug. 17, 1946.
[27] Biskind, M. S.: “DDT Poisoning and X Disease in Cattle”, J. Am. Vet. M. A. 114: 20, Jan. 1949.
[28] Biskind, M. S.: “DDT Poisoning a Serious Public Health Hazard”, Am. J. Dig. Dis. 16: 73, Feb. 1949.
[29] Biskind, M. S.: “DDT Poisoning and the Elusive ‘Virus X’: A New Cause for Gastro- Enteritis”, Am. J. Dig. Dis. 16: 79, March 1949.
[30] Boyd, C. L.: “A Report on “XX Disease in Texas”, J. Am. Vet. M. A. 113: 463, Nov. 1948.
[31] Cameron, C. R., and Burgess, F.: “The Toxicity of DDT”, Brit. M. J. 1: 865-871, June 23, 1945.
[32] Carte; R. H., Hubanks, P. E., et al: “Effect of Cooking on the DDT Content of Beef”, Science, 107: 347, April 2, 1948.
[33] Case, R. A. M.: Toxic Effects of DDT in Man”, Brit. M. J., 2: 842-845, Dec. 15, 1945.
[34] Council on Pharmacy and Chemistry, A. M. A.: “Health Hazards of Pesticides”, J. A. M. A. 137: 1603, Aug. 28, 1948.
[35] Crescitelli, F., and Gillman, A.: “Electrical Manifestations of Cerebellum and Cerebral Cortex Following DDT Administration to Cats and Monkeys”, Am. J. Physiol., 147: 127- 137, Sept. 1946.
[36] Deederer, C.: “DDT Toxicity”, M.Rec. 161: 216-220, April 1948
[37] Domenici, T. J.: “Hepatitis without Jaundice and without Hepatomegaly”, N. Eng. J. Med. 240: 88, Jan. 20, 1949
[38] Dunn, J. E., Dunn, J. C., and Smith, R. S.: “Skin Sensitising Properties of DDT for 31
Guinea Pig”, Pub. Health Rep. 61: 1614-1620, 1949.
[39] Editorial: Pesticides: “Chemical Contaminants of Foods”, J.A.M.A. 137: 1604, Aug. 28, 1948.
[40] Fitzhugh, O. G., and Nelson, A. A.: “The Chronic Oral Toxicity of DDT”, J. Pharm.acol. and Exper. Therap. 89: 18-30, Jan. 1947.
[41] Gamier, G.: “Treatment of Scabies with DDT”, .Presse Med. 56: 458, June 23, 1948. [42] Garett, ii. M., “Toxicity of DDT for Man”, Alabama St. M. A. J., 17: 74, Aug. 1947.
[43] Globus, J. H.: “DDT Poisoning; Histopathologic Observations on the Central Nervous System in So-Treated Monkeys, Dogs, Cats and Rats”, J. Neuropath. 7: 418-431, Oct. 1948.
[44] Haymaker, W., Ginzler, A. M., and Ferguson, J. L.: “Toxic Effects of Prolonged Ingestion of DDT on Dogs, with Special Reference to Lesions in Brain”, Am. J. M. Sc. 212: 423, Oct. 1946.
[45] Hill, K. R., and Daniiani, C. R.: “Death Following Exposure to DDT, Report of a Case”, New Eng. J. Med., 235: 897-899, Dec. 19, 1946.
[46] Hill, K. 3. and Robinson, G.: “A Fatal Case of DDT Poisoning in a Child, with an Account of Two Accidental Deaths in Dogs”. Brit. M. J. 2: 845-847, Dee. 15, 1945.
[47] Ingle, L.: “Toxicity of Chlordane to White Rats”, J. Econ. Entomol. 40: 264-268, 1947.
[48] Jandorf, B. J;. Sanett, H. P., and Bodansky, Oscar: “Effect of Oral Administration of DDT on Metabolism of Glucose and Pyruvie Acid in Rat Tissues”, J. Pharmaeol. and Exper. Therap. 88: 333-337, Dec. 1946.
[49] Jenkins, D. W.: “A Review of the Insecticide Hexachloro-cyclohexane (‘666’)”, Office of Technical Services, U. S. Dept of Commerce, Washington, D • C., No. PB 4034, Med. Div. Rept. No. 56, Sept. 26, 1945.
[50] Kempe, H. E.: “Progress Report on Benzene Hexachloride for the Destruction of Sheep Scab Mites”, Vet. Med., Feb. 1948, pp. 76-79.
[51] Kirk, H.: Vet. Red. 58: 43, 1946.
[52] Kirk, H.: “DDT in Canine Practice”, Vet. Med. Feb. 1947, PP. 76-78.
[53] Lawhon, G. J., Jr.: “X Disease in South Carolina”, N. Am. Vet. 29: 643, Oct. 1948.
[54] Leider, M.: “Allergenic Eczematous Contact-Type Dermatitis Caused by DDT”, J. Invest. Dermatol. 8: 125-126., March 1947.
[55] Lillie, R. D., Smith, M. I., and Stohlman, E. F.: Pathologic Action of DDT and Certain of its Analogs and Derivatives”, Arch. Path. 43: 127-142, Feb. 1947.
[56] Mackerras, I. M., and West, R. F. K.: “DDT Poisoning in Man”, M. J. Australia, 1: 400-401, March 23, 1946.
[57] Mobbs, J. F.:” Toxicity of Hexaehloroeyclohexane in Scabies, J.A.M.A. 138: 1253, Dec. 25, 1948. Personal Communication.
[58] Morrill, C. C.: “Hyperkeratosi.s or X Disease”, N. Am. Vet. 29: 642, Oct. 1948.
[59] Neal, P. A., Sweeney, T. B., Spicer, S. S., and von Oettingen, W. F.: “The Excretion of DDT in Man, Together with Clinical Observations”, Pub. Health Rep., 61: 403, March 22, 1946.
[60] Neal, P. A., von Oettingen, W. F., Smith, W. W., et al: Toxicology and Potential Dangers of Aerosols, Mists and Dusting Powders Containing DDT”, Pub. Health Rep. Suppl. 177, 1944.
[61] Neal, P. A., von Oettingeu, W. F., Dunn, R. C., and Sharpless, N. E.: “Toxicology and Potential Dangers of Aerosols and Residues from Aerosols Containing 3 Percent of DDT. Second Report, ibid., Suppl. 183, 1945.
[62] Nelson, A. A., Draize, 3. H., Woodard, G., et al: “Histopathological Changes Following Administration of DDT to Several Species of Animals”, U. S. Pub. Health Rep. 59: 1009, Aug. 4, 1944.
[63] Neve, Helen: “Toxic Effects of DDT on a Cat”, Vet. Rec. 58: 43, 1946. Vet. Med., Feb. 1947, p. 78.
[64] Niedelman, M. L.: “Contact Dermatitis Due to DDT”, Occup. Med. 1: 391-395, April 1946.
[65] Radeleff, R. D.: “DDT Spray Outmodes Dipping Vat”, Vet. Med. Oct. 1947, pp. 372- 373.
[66] Radeleff, R. D.: “Chlordane Poisoning: Symptomatology and Pathology, Vet. Med. Aug. 1948, pp. 342-347.
[67] Robinson, J. H.: “Harvest Analysis of DDT Residues”, Food Packer, 29: 50-53, 1948.
[68] Riker, W. F., Jr., Huebner, Virginia, R., Raska, S. B., and Cattell, McKeen: “Studies on DDT, Effects on Oxidative Metabolism”, J. Pharmacol. and, Exper. Therap., 88: 327- 332, Dec. 1946.
[69] Sarrett, H. P., and Jandorf, B. J.: “Effects of Chronic DDT Intoxication in Rats on Lipids and Other Constituents of Liver”, ibid., 91: 340-344, Dec. 1947.
[70] Smith, M. I.: “Accidental Ingestion of DDT, with a Note on its Metabolism in Man”, J.A.M.A., 131: 519-520, Juno 8, 1946.
[71] Smith, M. I., and Stohlnian, E. F.: “Pharmacologic Action of 2, 2 his (p-Chlorophenyl) 1,1,1-Trichloroethane and its Estimation in the Tissues and Body Fluid”, Pub. Health Rep., 59: 984, July 28, 1944.
[72] SmIth, M. I., and Stohlman, E. F.: “Further Studies on the Pharmacologic Action of DDT”, ibid., 60: 289, March 16, 1945.
[73] Smith, N. 3.: “Death Following Accidental Ingestion of DDT”, J.A.M.A., 136: 469- 471, Feb. 14, 1948.
[74] Smith, R. F., Fullmes, O. H., and Messenger, P. S.: “DDT Residues on Alfalfa Hay and Seed Chaff”, J. Econ. Entomol. 41: 755-8, 1948.
[75] Strycker, G. V., and Godfroy, B.: “Dermatitis Resulting from Exposure to DDT”, J. Missouri St. M. A., 43: 384-386, June 1948.
[76] Taylor, E. L.: “Danger of Ununction with DDT”, Lancet, 2: 320, Sept. 8, 1945.
[77] Telford, H. S., and Guthrie, J. E.: “Transmission of the Toxicity of DDT Through the Milk of White Rats and Goats”, Science, 102: 647, Dec. 21, 1945.
[78] Thoungh, TI. C.: “Poisonous Effects of DDT on Humans”, Indian M. Ga:. 81: 432, Oct. 1946.
[79] U. S. Dept. Agriculture, “Bureau of Entomology and Plant Quarantine: Now Insecticides in Grasshopper Control”, Bull. E-722, May 1947. Bull. EC.1, March 1948.
[80] U. S. Dept. Agriculture, Bureau of Entomology and Plant Quarantine: “New Insecticides for Controlling External Parasites of Livestock”, Bull. E. 762, Dec. 1948.
[81] Westerfteld, C.: “The Use of DDT in Medicine-A Review”, Vet. Med., Oct. 1946, pp. 355-360.
[82] Wigglesworth, V. D.: “A Case of DDT Poisoning in Man”, Brit M. J. 1: 517, April 14, 1945.
[83] Wilson, J. B.: Are Pesticides Making Your Food Unsafer? Hygiea, Jan. 1949. p. 44.
[84] Woodard, G., Ofner, Ruth B., and Montgomery, C. M.: “Accumulation of DDT in the Body Fat and its Appearance in the Milk of Dogs”, Science, 102: 177-178, Aug. 17, 1945.
[85] Wright, C. S., Doan, C. A., and Haynie, H. C.: “Agranulocytosis Occurring after Exposure to DDT Pyrethrum Aerosol Bomb”, Am. J. Med., 1: 562-567, Nov. 1946.
[86] The Pesticide Residues Amendment of 1954, Pub. L. No. 83-518, ch. 559, 68 Stat. 511 [codified at 21 USC § 346a (1981)]; and the Food Additives Amendments of 1958, Pub. L. No. 85-529, Ch. 4.72 Stat. 1785 [codified at 21 USC § 348 (1981)], respectively.
[87] 20 Fed. Reg. 750 (1955) [codified until repealed at 21 CFR § 120. 1(f) (1956). [88] DDT Regulatory History: A Brief Survey (to 1975). United States Environmental
Protection Agency (EPA).
[89] Ibid.
[90] TIME Magazine, U.S. Edition, March 14, 1994 Vol. 143 No. 11.
(91] Handbook of Pesticide Toxicology, edited by Wayland J. Hayes, Jr. and Edward R. Laws, Academic Press Inc., Harcourt Brace Jovanovich, Publishers, San Diego, 1991.
[92] Peter Duesberg and Brian J. Ellison, Inventing the AIDS Virus, Regnery Pub.,1996. [93] Ibid.
[94] Biskind, MS (1953) “Public Health Aspects of the New Insecticides,” American Journal of Digestive Diseases 20: 331-341.
[95] Peter Duesberg and Brian J. Ellison, Inventing the AIDS Virus, Regnery Pub.,1996. [96] DDT Regulatory History: A Brief Survey (to 1975). United States Environmental
Protection Agency (EPA).
[97] Poliomyelitis: Fact sheet N°114″. World Health Organization. Sep 2016. Retrieved 14 Sep 2016.
[98] Ibid.
[99] DDT Regulatory History: A Brief Survey (to 1975). United States Environmental
Protection Agency (EPA).
[100] Ibid.
[101] Handbook of Pesticide Toxicology, edited by Wayland J. Hayes, Jr. and Edward R.
Laws, Academic Press Inc., Harcourt Brace Jovanovich, Publishers, San Diego, 1991.
[102] Rea WJ, Johnson AR, Fenyves E, Butler J. Related Articles: The environmental aspects of the post-polio syndrome. Birth Defects Orig Artic Ser. 1987;23(4):173-81. No abstract available. Pub Med ID: 3620615; UI: 87299998.
[103] Ibid.
[104] Casarett and Doull’s Toxicology (1996).
[105) Rea WJ, Johnson AR, Fenyves E, Butler J. Related Articles: The environmental aspects of the post-polio syndrome. Birth Defects Orig Artic Ser. 1987;23(4):173-81. No abstract available. Pub Med ID: 3620615; UI: 87299998.
[106] PubMed ID: 7611631, UI: 95336052 (London, May, 1995)
[107] Pub Med ID: 7611630, UI: 95336051 (Bethesda, MA, May, 1995)
[108] Pub Med ID: 8818905, UI: 96415998 (Lyon, France, Aug., 1996)
[109] Alfredo Morabia (1 January 2004). A History of Epidemiologic Methods and Concepts. Springer. pp. 133–4. ISBN 978-3-7643-6818-0. Retrieved 22 June 2013.
[110] Ibid.
[111] Morton S. Biskind, MD. “Public Health Aspects of the New Insecticides”. American
Journal of Digestive Diseases, New York, 1953, v 20, p331. [112] Ibid.
[113] Young RO (2016) Second Thoughts Concerning Viruses, Vaccines and the HIV/AIDS Hypothesis – Part 2. Int J Vaccines Vaccin 2(3): 00034. DOI: 10.15406/ijvv.2016.02.00034
[114] Dirt and Disease: Polio before FDR Rutgers University Press, 1992. [115] Ibid.
[116] Menkes, John H., Child Neurology, pg. 420, (1995).
[117] A Paralyzing Fear: The Story of Polio in America. Produced by Paul Wagner, Nina Gilden Seavey. Directed, written by Nina Gilden Seavey. Narration written by Stephen Chodorov. With: Narrator: Olympia Dukakis. Camera (Colorlab color), Allen Moore, Reuben Aaronson; editor, Catherine Shields; music, Paul Christianson; associate producers, Tom Wentworth, Malvina Anderson Martin. Reviewed on videocassette, N.Y., March 3, 1998. Running time: 90 min.
[118] FILM REVIEW; Once a Fear Beyond Fear Itself, by STEPHEN HOLDEN, Published: March 4, 1998, New York Times.
[119] Ibid.
[120] Duesberg, Peter and Ellison, Brian J., Inventing the AIDS Virus, Regnery Pub.,1996.
[121] Ibid.
[122] Ibid.
[123] Ibid.
[124] Ibid.
[125] Rose DR (2004). “Fact Sheet—Polio Vaccine Field Trial of 1954.” March of Dimes Archives. (2004).
[126] Ibid.
[127] American Journal of Digestive Diseases, 1953 20:330 [128] Ibid.
[129] Ibid.
[130] Jenkins, D. W.: “A Review of the Insecticide Hexachloro-cyclohexane (‘666’)”, Office of Technical Services, U. S. Department of Commerce, Washington, D.C., No. PB 4034, Med. Div. Rept. No. 56, Sept. 26, 1945.
[131] Biskind, M., “DDT Poisoning and the Elusive ‘Virus X’.” A New Cause for Gastroenteritis.” Am. J. Dig., Vol. 16, Num 3, pg. 79-84, (1949).
[132] Biskind, MS, Bieber, I, “DDT Poisoning A New Syndrome With Neuropsychiatric Manifestations,” American Journal of Psychotherapy, p261, (1949).
[133] Presented before the Select Committee to Investigate the Use of Chemicals in Food Products, United States House of Representatives, U.S. December 12, 1950 Westport, Conn.
[134] “Salk and Sabin: poliomyelitis immunisation”. J Neurol Neurosurg Psychiatry. 75 (11): 1552. doi:10.1136/jnnp.2003.028530. PMC 1738787. PMID 15489385.
[135] H. Rept. No. 2356, 82d Cong., 2d sess. 1 (1952), reprinted in A Legislative History of the Federal Food, Drug and Cosmetic Act and Its Amendments 499 (hereinafter Legislative History)
[136] Scobey, RR, “Is The Public Health Law Responsible For The Poliomyelitis Mystery?” Syracuse, N.Y., Archive of Pediatrics (May, 1951).
[137] White, Mark; Sharon M. McDonnell; Denise H.Werker; Victor M. Cardenas; Stephen B. Thacker (2001). “Partnerships in International Applied Epidemiology Training and Service,”. American Journal of Epidemiology 154 (11): 993–999. doi:10.1093/aje/154.11.993.
[138] Van Nostrand’s Encyclopedia of Science and Engineering, Van Nostrand Reinhold 1995, v 5, p1775
[139] “Salk and Sabin: poliomyelitis immunisation”. J Neurol Neurosurg Psychiatry. 75 (11): 1552. doi:10.1136/jnnp.2003.028530. PMC 1738787. PMID 15489385.
[140] Ralph R. Scobey, MD. “The Poison Cause of Poliomyelitis and Obstructions to Its Investigation.” Archive of Pediatrics, April 1952.
[141] The National Adipose Tissue Survey, reported in Handbook of Pesticide Toxicology, edited by Wayland J. Hayes, Jr. and Edward R. Laws, Academic Press Inc., Harcourt Brace Jovanovich, Publishers, San Diego, 1991, pg. 303.
[142] The National Adipose Tissue Survey, reported in Handbook of Pesticide Toxicology, edited by Wayland J. Hayes, Jr. and Edward R. Laws, Academic Press Inc., Harcourt Brace Jovanovich, Publishers, San Diego, 1991, pg. 303.
[143] Van Nostrand’s Encyclopedia of Science and Engineering (1995), vol. 5, pg.1725. [144] Offit, Paul A. (2007). The Cutter Incident: How America’s First Polio Vaccine Led to
the Growing Vaccine Crisis. Yale University Press. p. 38. ISBN 0-300-12605-0. [145] Albert Sabin to Henry Kumm, Sabin Papers, UC, Pittsburgh Press, 1954. [146] American Journal of Digestive Diseases, 1953 20:330.
[147] Trevelyan, B., Smallman-Raynor, M. and Cliff, A.D., The Spatial Dynamics of Poliomyelitis in the United States: From Epidemic Emergence to Vaccine-Induced Retreat, 1910–1971, Ann Assoc Am Geogr. 2005 Jun; 95(2): 269–293.
[148] Baicus, A., History of Polio Vaccination, World J Virol. 2012 Aug 12; 1(4): 108–114. Published online 2012 Aug 12. doi: 10.5501/wjv.v1.i4.108.
[149] Ibid.
[150] Women’s History Month: “Oveta Culp Hobby” by Senator Kay Bailey Hutchison
Humanities Texas, March 2012.
[151] Harry M. Marks, “The 1954 Salk Poliomyelitis Vaccine Field Trial,” Institute of the History of Medicine, Johns Hopkins University, Baltimore, MD: 2008.
152[ National Museum of American History, “Whatever Happened to Polio?” Time line, http://americanhistory.si.edu/polio/timeline/index.htm (accessed March 28,, 2012).
[153] Abid.
[154] Norrby E., Prusiner S.B., Polio and Nobel Prizes: looking vack 50 years. Ann Neurol.
2007 May;61(5):385-95.
[155] Eloise Batic, You Are There 1955: Ending Polio exhibit text (2012).
[156] Boston Herald newspaper, April 18, 1955, “Drug Companies Expecting Big Profit on
Salk Vaccine”,
[157] Washington Bureau of the Detroit Free Press reports, June 3, 1955.
[158] Michigan University. Poliomyelitis Evaluation Center (1955), An evaluation mof the 1954 poliomyelitis vaccine trials; summary report. Ann Arbor: n.p. , pp. 17-18 as quoted in Marks, Harry M. “The 1954 Salk Poliomyelitis Vaccine Field Trial.” Institute of the History of Medicine, Johns Hopkins University. Baltimore: 2008, p. 20.
[160] McBean E. The Poisoned Needle. Mokelumne Hill, California: Health Research,1957:1
[161] McBean E. The Poisoned Needle. Mokelumne Hill, California: Health Research, 1957:119.
[162] McBean E. The Poisoned Needle. Mokelumne Hill, California: Health Research,1957:1
[163] Offit, Paul A. The Cutter Incident: How America’s First Polio Vaccine Led to the Growing Vaccine Crisis, Yale University Press, 2005, pp. 100, 116–19, 133. ISBN 0-300- 10864-8
[164] Ibid.
[165] Smith, JS, “Patenting the Sun: Polio and the Salk Vaccine,” 1st Edition, William
Morrow & Co; 1st edition (April 1990).
[166] Offit PA (2005), “The Cutter incident, 50 years later” (PDF). N. Engl. J. Med. 352 (14): 1411–1412. doi:10.1056/NEJMp048180. PMID 15814877
[167] McBean E., The Poisoned Needle. Mokelumne Hill, California: Health Research,1957:1.
[168] Harris RJ et al Contaminant viruses in two live vaccines produced in chick cells. J Hyg (London) 1966 Mar:64(1) : 1-7
[169] McBean E. The Poisoned Needle. Mokelumne Hill, California: Health Research,1957:1
[170] Ibid.
[171] Ibid.
[172] Ibid.
[173] Ii. Results. American journal of public health and the nation’s health. 1955;45:15–48. [PMC free article] [PubMed]
[174] Harper’s Magazine. “’Who is responsible, and why, for the chaotic confusion over the polio inoculations?’ A noted medical journalist disentangles the essential facts.” August, 1955.
[175] Ibid.
[176] Ibid.
[177] American Cancer Society, Volume 8, Issue 1, Pages 1–218, (1955).
[178] Paul JR. A history of poliomyelitis. New Haven, CT: Yale University Press; 1971.
[179] Ibid.
[180] Ibid.
[181] Ibid.
[182] Rogers N. Dirt and disease: Polio before fdr. New Brunswick, NJ: Rutgers University Press; 1992.
[183] Ibid.
[184] Smith, Derek R; Leggat Peter A (2005). “Pioneering figures in medicine: Albert Bruce Sabin–inventor of the oral polio vaccine”. The Kurume medical journal. 52 (3): 111–6. doi:10.2739/kurumemedj.52.111. PMID 16422178
[185] Rose, David, March of Dimes Archives, August 26, 2010. http://www.marchofdimes.org/mission/a-history-of-the-march-of-dimes.aspx
[186] American Journal of Public Health and the Nations Health: May 1956, Vol. 46, No. 5: 547–562. Citation | PDF (2177 KB) | PDF Plus (744 KB)
[187]
[188] Sweet BH, Hilleman MR. The Vacuolating Virus: SV-40. As cited in The polio vaccine and simian virus 40 by Moriarty, T.J. http://www.chronicillnet.org/online/bensweet.html
[189] O’Hern M. Profiles: Pioneer Women Scientists. Bethesda, MD: National Institutes of Health.
[190] Curtis T, Manson P. Scientist’s Polio Fear Unheeded: How U.S. Researcher’s Warning Was Silenced. The Houston Post 1992:A1 and A12.
[191] Sweet BH, Hilleman MR. The Vacuolating Virus: SV-40. As cited in The polio vaccine and simian virus 40 by Moriarty, T.J. http://www.chronicillnet.org/online/bensweet.html
[192] Moriarty T.J. The polio vaccine and simian virus 40. Online News Index.
http://www.chronicillnet.org/online/bensweet.html
[193] Shah K, Nathanson N. Human exposure to SV40. American Journal of Epidemiology, 1976;103:1-12.
[194] Curtis T. The origin of AIDS: A startling new theory attempts to answer the question, “Was it an act of God or an act of man”, Rolling Stone, March 19,1992:57.
[195] Bookchin D, Schumaker J. Tainted Polio Vaccine Still Carries Its Threat 40 Years Later. The Boston Globe, January 26, 1997.
[196] Innis MD. Oncogenesis and poliomyelitis vaccine. Nature, 1968;219:972–3. [197] Soriano F, et al. Simian virus 40 in a human cancer. Nature, 1974; 249:421–4.
[198] Weiss AF, et al. Simian virus 40-related antigens in three human meningiomas with defined chromosome loss. Proceedings of the National Academy of Science, 1975;72(2):609–13.
[199] Scherneck S, et al. Isolation of a SV-40-like papovavirus from a human glioblastoma. International Journal of Cancer, 1979;24:523–31.
[200] Stoian M, et al. Possible relation between viruses and oromaxillofacial tumors. II. Research on the presence of SV40 antigen and specific antibodies in patients with oromaxillofacial tumors. Virologie, 1987;38:35–40.
[201] Stoian M, et al. Possible relation between viruses and oromaxillofacial tumors. II. Detection of SV40 antigen and of anti-SV40 antibodies in patients with parotid gland tumors. Virologie, 1987;38:41–6.
[202] Bravo MP, et al. Association between the occurrence of antibodies to simian vacuolating virus 40 and bladder cancer in male smokers. Neoplasma, 1988;35:285–8.
[203] O’Connell K, et al. Endothelial cells transformed by SV40 T-antigen causeKaposi’s sarcoma-like tumors in nude mice. American Journal of Pathology, 1991;139(4):743–9.
[204] Weiner LP, et al. Isolation of virus related to SV40 from patients with progressive multifocal leukoencephalopathy. New England Journal of Medicine, 1972;286:385–90.
[205] Tabuchi K. Screening of human brain tumors for SV-40-related T-antigen. International Journal of Cancer 1978;21:12–7.
[206] Meinke W, et al. Simian virus 40-related DNA sequences in a human brain tumor. Neurology 1979;29:1590–4.
[207] Krieg P, et al. Episomal simian virus 40 genomes in human brain tumors. Proceedings of the National Academy of Science 1981; 78:6446-50.
[208] Krieg P, et al. Cloning of SV40 genomes from human brain tumors. Virology 1984;138:336–40.
[209] Geissler E. SV40 in human intracranial tumors: passenger virus or oncogenic >hit- and-run= agent? Z Klin Med, 1986;41:493–5.
[210] Geissler E. SV40 and human brain tumors. Progress in Medical Virology, 1990;37:211–22.
[211] Bergsagel DJ, et al. DNA sequences similar to those of simian virus 40 in ependymomas and choroid plexus tumors of childhood. New England Journal of Medicine, 1992;326:988–93.
[212] Martini, M., et al. Human brain tumors and simian virus 40. Journal of the National Cancer Institute, 1995;87(17):1331.
[213] Lednicky JA, et al. Natural Simian Virus 40 Strains are Present in Human Choroid Plexus and Ependymoma Tumors. Virology, 1995;212(2):710–7.
[214] Tognon M, et al. Large T Antigen Coding Sequence of Two DNA Tumor Viruses, BK and SV-40, and Nonrandom Chromosome Changes in Two Gioblastoma Cell Lines. Cancer Genetics and Cytogenics, 1996;90(1): 17–23.
[215] Vilchez RA, et al. Association between simian virus 40 and non-hodgkin lymphoma. Lancet, (March 9, 2002), 359: 817–23.
[216] Carbone, M., et al. SV-40 Like Sequences in Human Bone Tumors. Oncogene, 1996;13(3):527–35.
[217] Pass, HI, Carbone, M., et al. Evidence For and Implications of SV-40 Like Sequences in Human Mesotheliomas. Important Advances in Oncology, 1996:89-108.
[218] Rock, Andrea. The Lethal Dangers of the Billion Dollar Vaccine Business, Money, December 1996:161.
[219] Carlsen, W. Rogue virus in the vaccine: Early polio vaccine harbored virus now feared to cause cancer in humans. San Francisco Chronicle, July 15,2001:7. Research by Susan Fisher, epidemiologist, Loyola UniversityMedical Center.
[220] National Institutes of Health. Zones of Contamination: Globe Staff Graphic.
[221] Bookchin D, Schumacher J. Tainted polio vaccine still carries its threat 40 years later. The Boston Globe, January 26, 1997.
[222] SV-40 Contamination of Polio Vaccine. Well Within Online, (February 3,2001, updated). http://www.nccn.net/~wwithin/polio.htm
[223] Rosa FW, et al. Absence of antibody response to simian virus 40 afterinoculation with killed-poliovirus vaccine of mothers offspring with neurological tumors. New England Journal of Medicine, 1988;318:1469.
[224] Rosa FW, et al. Response to: Neurological tumors in offspring after inoculation of mothers with killed poliovirus vaccine. New England Journal of Medicine, 1988, 319:1226.
[225] Martini F, et al. SV-40 Early Region and Large T Antigen in Human Brain Tumors, Peripheral Blood Cells, and Sperm Fluids from Healthy Individuals. Cancer Research, 1996;56(20):4820–5.
[226] Fisher, Barbara. Vaccine safety consumer group cites conflict of interest in government report on cancer and contaminated polio vaccine link. National Vaccine Information Center (NVIC); Press Release, January 27, 1998.
[227] National Cancer Institute (June 2001).
[228] The Landsteiner and Popper study, first published in Germany, was reported in Robert W Lovett, MD. The Occurrence of Infantile Paralysis in Massachusetts in 1908. Boston Medical and Surgical Journal, pg. 112, July 22, 1909.
[229] Young, RO (2016) Second Thoughts about Viruses, Vaccines, and the HIV/AIDS Hypothesis – Part 1. Int J Vaccines Vaccin 2(3): 00032. DOI: 10.15406/ijvv.2016.02.00032
[230] Young, RO (2016) Second Thoughts Concerning Viruses, Vaccines and the HIV/AIDS Hypothesis – Part 2. Int J Vaccines Vaccin 2(3): 00034. DOI: 10.15406/ijvv.2016.02.00034
[231] Young RO (2016) Second Thoughts Concerning Viruses, Vaccines and the HIV/AIDS Hypothesis – Part 3 HIV/AIDS and the Monomorphic Disease Model. Int J Vaccines Vaccin 2(3): 00035. DOI: 10.15406/ijvv.2016.02.00035
[232] Young RO (2016) Who Had Their Finger on the Magic of Life – Antoine Bechamp or Louis Pasteur?. Int J Vaccines Vaccin 2(5): 00047. DOI: 10.15406/ijvv.2016.02.00047
[233] Peter Duesberg and Brian J. Ellison, Inventing the AIDS Virus, Regnery Pub., 1996. [234] Gerald L. Geison, The Private Science Of Louis Pasteur, Princeton University Press, 1995.
[235] The Landsteiner and Popper study, first published in Germany, was reported in Robert W Lovett, MD. The Occurrence of Infantile Paralysis in Massachusetts in 1908. Boston Medical and Surgical Journal, pg. 112, July 22, 1909.
[236] Shaw D. Unintended casualties in war on polio. Philadelphia Inquirer June 6, 1993:A1.
[237] Moriarty T.J. The polio vaccine and simian virus 40. Online News Index. http://www.chronicillnet.org/online/bensweet.html
[238] Koprowksi H. Tin anniversary of the development of live virus vaccine. Journal of the American Medical Association 1960;174:972–6.
[239] Hayflick L, Koprowski H, et al. Preparation of poliovirus vaccines in a human fetal diploid cell strain. American J Hyg 1962;75:240–58.
[240] Hayflick L, Koprowski H, et al. Preparation of poliovirus vaccines in a human fetal diploid cell strain. American J Hyg 1962;75:240–58.
[241] Koprowski H. In a letter sent to the Congressional Health and Safety Subcommittee, April 14, 1961.
[242] Rock, Andrea. The Lethal Dangers of the Billion Dollar Vaccine Business, Money, December 1996:161.
[243] Scheibner V. Vaccination: 100 Years of Orthodox Research Shows that Vaccines represent a Medical Assault on the Immune System. Blackheath, NSW, Australia: Scheibner Publications, 1993153.
[244] Curtis T. Expert says test vaccine: backs check of polio stocks for AIDS virus. The Houston Post, March 22, 1992:A-21.
[245] Carlsen, W. Rogue virus in the vaccine: Early polio vaccine harbored virus now feared to cause cancer in humans. San Francisco Chronicle, July 15,2001:7. Research by Susan Fisher, epidemiologist, Loyola UniversityMedical Center.
[246] Neustaedter R. The Vaccine Guide. Berkeley, California: North Atlantic Books, 1996:107–8
[247] Curtis T. Expert says test vaccine: backs check of polio stocks for AIDS virus. The Houston Post, March 22, 1992:A-21.
[248] Essex M, et al. The origin of the AIDS virus. Scientific American, 1988; 259:64–71. [249] Karpas A. Origin and Spread of AIDS. Nature, 1990; 348:578.
[250] Kyle WS. Simian retroviruses, poliovaccine, and origin of AIDS. Lancet, 1992; 339:600–1.
[251] Elswood BF, Stricker RB. Polio vaccines and the origin of AIDS. Medical Hypothesis, 1994:42:347–54.
[252] Myers G, et al. The emergence of simian/human immunodeficiency viruses. AIDS Res Human Retro 1992:8:373–86.
[253] Curtis T. The origin of AIDS: A startling new theory attempts to answer the question “Was it an act of God or an act of man”, Rolling Stone, March 19,1992:57.
[254] O’Hern M. Profiles: Pioneer Women Scientists. Bethesda, MD: National Institutes of Health.
[255] Curtis T. Expert says test vaccine: backs check of polio stocks for AIDS virus. The Houston Post, March 22, 1992:A-21.
[256] Curtis T. Expert says test vaccine: backs check of polio stocks for AIDS virus. The Houston Post, March 22, 1992:A-21.
[257] Essex M, et al. The origin of the AIDS virus. Scientific American, 1988; 259:64–71. [258] Karpas A. Origin and Spread of AIDS. Nature, 1990; 348:578.
[259] Kyle WS. Simian retroviruses, poliovaccine, and origin of AIDS. Lancet, 1992; 339:600–1.
[260] Elswood BF, Stricker RB. Polio vaccines and the origin of AIDS. Medical Hypothesis, 1994:42:347–54.
[261] Workshop on Simian Virus-40 (SV-40): A Possible Human Polyomavirus. National Vaccine Information Center, January 27-28, 1997. http://www.909shot.com/polio197.htm (Includes a summary of evidence presented at the Eighth Annual Houston Conference on AIDS.)
[262] Martin B. Polio vaccines and the origin of AIDS: The career of a threatening idea. Townsend Letter for Doctors, January 1994:97–100.
[263] Curtis T. Did a polio vaccine experiment unleash AIDS in Africa? The Washington Post, April 5, 1992:C3+.
[264] Myers G, et al. The emergence of simian/human immunodeficiency viruses. AIDS Res Human Retro 1992:8:373–86.
[265] World Health Organization. T-lymphotropic retroviruses of nonhuman primates. WHO informal meeting. Weekly Epidemiology Records, 1985; 30:269–70.
[266] Ibid.
[267] Elswood BF, Stricker RB. Polio vaccines and the origin of AIDS. Medical
Hypothesis, 1994:42:347–54.
[268] Ohta Y, et al. No evidence for the contamination of live oral poliomyelitis vaccines with simian immunodeficiency virus. AIDS, 1989; 3:183–5.
[269] Huet T, et al. Genetic organization of a chimpanzee lentivirus related to HIV-1. Nature, 1990; 345:356–9.
[270] Desrosiers RC. HIV-1 origins: A finger on the missing link. Nature, 1990;345:288– 9.
[271] Sabin AB. Properties and behavior of orally administered attenuated poliovirus vaccine. Journal of the American Medical Association, 1957; 164:1216–23.
[272] Siehe Ausführungen zu Virchows Leben und Wirkung in WissenschafftPlus Nr. 5/2015 und Nr. 6/2015. 2 Anticontagionism between 1821 and 1867.
[273] Aufsatz von Erwin H. Ackerknecht in der Zeitschrift Bulletin of the History of Medicine, Volume XXII, The Johns Hopkins Press, 1948.
[274] Bech V, Magnus Pv. Studies on measles virus in monkey kidney tissue cultures. Acta Pathol Microbiol Scand. 1959; 42 (1): 75–85.
[275] Nakai M, Imagawa DT. Electron microscopy of measels virus replication. J. Virol. 1969 Feb; 3v (2): 187–97.
[276] Lund GA, Tyrell, DL, Bradley RD, Scraba DG. The molecular length of measles virus RNA and the structural organization of measles nucleocapsids. J. Gen. Virol. 1984 Sep;65 (Pt 9): 1535–42.
[277] Daikoku E, Morita C, Kohno T, Sano K. Analysis of Morphology and Infectivity of Measles Virus Particles. Bulletin of the Osaka Medical College. 2007; 53 (2): 107–14.
[278] Horikami SM, Moyer SA. Structure, Transcription, and Replication of Measles Virus. Curr Top Microbiol Immunol. 1995; 191: 35–50.
[279] Siehe WissenschafftPlus Nr. 1/2014.
[280] Zur Geschichte der frühen Virusforschung. Übersichtsarbeit von Prof. Karlheinz Lüdtke. Reprint 125 des MAX-PLANCK-INSTITUT FÜR WISSENSCHAFTSGESCHICHTE, 89 Seiten, 1999.



















































You must be logged in to post a comment.